







- En
- Fr
- عربي





Who Killed Solidarity? The Political Economy of Health Financing Collapse in Lebanon and Fragile States
Who Killed Solidarity? The Political Economy of Health Financing Collapse in Lebanon and Fragile States
Introduction
Lebanon’s health system collapse since 2019 is commonly described as a direct consequence of macroeconomic failure: currency depreciation, fiscal insolvency, and state paralysis. While these shocks accelerated the breakdown, such explanations are incomplete. They obscure a more uncomfortable reality: Lebanon’s health financing system did not fail accidentally; it was engineered to remain fragile. Long before the financial crash, its architecture reflected deliberate political calculations that prioritized patronage, fragmentation, and selective protection over solidarity and universalism. The crisis did not create these failures--it exposed them.
In politically fragmented states, financing arrangements often become tools of power rather than instruments of redistribution. Lebanon represents an extreme case of this dynamic. Despite total health expenditures exceeding 8% of GDP prior to 2019, Lebanon consistently failed to translate spending into equitable access or financial protection. Access to care varied sharply by employment status, geography, and political affiliation. Out-of-pocket payments accounted for approximately 34 - 38% of total health expenditure between 2010 and 2018, a level the WHO associates with a high probability of catastrophic health spending.
This article argues that Lebanon’s health financing system functioned as a political instrument, enabling political actors to retain broad discretion over access while avoiding binding commitments to universal risk pooling. Multiple insurance schemes--public, semi-public, and private--operated in parallel with minimal coordination, creating space for selective allocation of benefits and reducing the fiscal and political pressures associated with comprehensive pooling. The Ministry of Public Health was positioned primarily as a payer of last resort role rather than empowered as a strategic purchaser, and sector organizer, while regulatory oversight of private providers remained weak by design. Together, these arrangements enabled dominant political actors to sustain narratives of social protection while shifting a substantial share of financial risk onto households.
The economic collapse transformed these long-standing vulnerabilities into systemic failure. Currency devaluation eroded the real value of public reimbursements, hospitals curtailed services or closed, health workers emigrated, and households absorbed catastrophic health expenditures. Yet the speed and severity of the collapse cannot be explained by economic shock alone. Health systems with stronger pooling arrangements, clearer purchasing authority, and institutionalized solidarity mechanisms demonstrated greater resilience under comparable stress. Lebanon’s did not--because collective protection was never its organizing principle.
By situating Lebanon’s experience within the political economy of health financing, this article challenges technocratic narratives that frame reform primarily as a matter of efficiency, cost containment, or benefit package design. Instead, it demonstrates how financing arrangements reflect underlying power relations, institutional incentives, and distributive conflicts. Drawing on political economy frameworks developed by the World Health Organization and applied in fragile and conflict-affected settings, the analysis focuses on four interacting dimensions: actor politics, budget politics, leadership dynamics, and external influence. Together, these forces shaped financing decisions that undermined risk pooling and entrenched inequality.
Lebanon also offers broader theoretical relevance. Unlike many fragile states, Lebanon combined a relatively sophisticated private healthcare market with a weak and fragmented public financing architecture. This hybrid model allowed costs to be externalized while access remained stratified. The result was not underdevelopment but selective institutional development, where health services expanded without corresponding solidarity mechanisms. This makes Lebanon an instructive case for understanding how middle-income countries can exhibit advanced service provision alongside extreme financing inequities.
The core question is deliberately narrow: why did Lebanon’s health financing system collapse so completely, and who was protected when it did? By tracing how financing mechanisms were structured, captured, and ultimately allowed to fail under crisis, the analysis shows that collapse was not a policy accident but a politically survivable outcome. Restoring solidarity, therefore, is not primarily a technical challenge - it requires political and institutional realignment to ensure that health financing serves shared protection rather than discretionary control.

Chapter One
Conceptual Framework: Political Economy of Health Financing
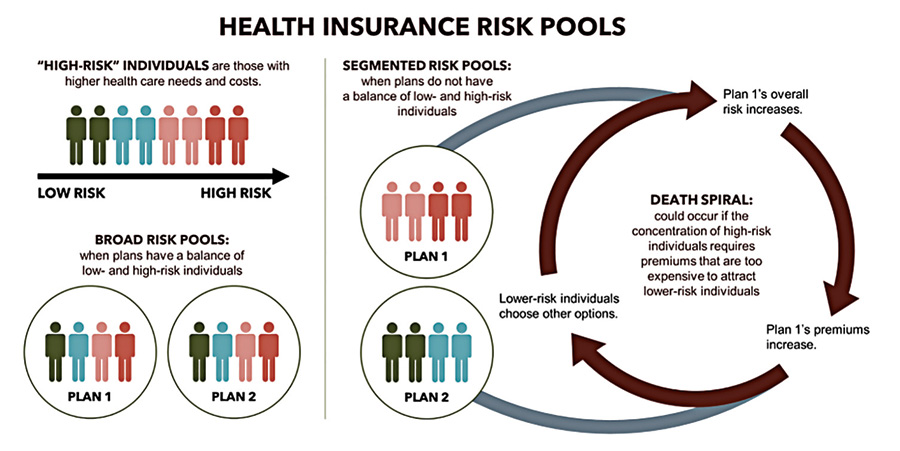
Health financing lies at the core of any health system’s capacity to deliver equitable, sustainable, and effective care. The World Health Organization defines its core functions as revenue raising, pooling, and purchasing, supported by benefit design and governance arrangements that determine who is covered, for which services, and under what conditions1. Together, these functions determine whether health systems protect households from financial hardship or expose them to catastrophic expenditure. Health financing is therefore not merely a technical subsystem; it is the institutional expression of solidarity--or its absence.
Revenue raising, pooling, purchasing, and benefit design together determine how financial risk is distributed across a population. When aligned toward collective risk-sharing, these functions advance Universal Health Coverage (UHC): access to needed health services of sufficient quality without financial hardship (WHO, 2010). When fragmented, underfunded, or selectively applied, they reproduce inequality, exclusion, and financial vulnerability.
The political economy of health financing seeks to make these dynamics explicit. Political economy analysis examines how political actors, economic interests, and institutional arrangements interact to shape policy outcomes. In health financing, this approach shifts attention beyond optimal design toward questions of control, incentives, and persistence: who controls resources, who influences decisions, and why inefficient or inequitable arrangements persist despite sustained evidence of harm2. Health financing systems are embedded within broader governance structures and cannot be meaningfully reformed in isolation from them.
At its core, political economy analysis focuses on four interrelated elements: stakeholders, power, interests, and institutions. Stakeholders include state actors, private providers, insurers, political elites, donors, and citizens, each possessing unequal formal and informal power to shape financing decisions. Interests may align or conflict depending on how financing arrangements affect revenue streams, political legitimacy, or access to rents.
Institutions--both formal (laws, regulations, budgets) and informal (patronage networks, sectarian norms, professional hierarchies)--structure how these interests are expressed and sustained over time3.
Crucially, political economy analysis rejects the assumption that dysfunctional health financing systems persist primarily due to technical incapacity or poor design. Instead, it emphasizes that such systems often represent stable political equilibria that benefit influential actors even as they generate inefficiencies and inequities4. Reform failure is thus often better explained by political resistance than by technical complexity. This perspective is essential for understanding why fragmented pooling arrangements, regressive financing mechanisms, and weak purchasing systems persist in many low - and middle - income countries, including Lebanon.
To operationalize political economy analysis in health financing, the World Health Organization has developed a structured methodological approach. The WHO Political Economy Analysis for Health Financing framework identifies key analytical domains that should be examined in any reform context to uncover the political drivers of financing outcomes5. Rather than offering a prescriptive model, the framework provides a structured way to analyze how political dynamics shape reform trajectories.
One central domain is actor politics, which examines the roles, interests, and relative power of stakeholders involved in health financing. This includes identifying reform champions and veto players, mapping alliances and conflicts (Sparkes et al., 2019). In fragile states, actor politics often extends beyond formal institutions to include sectarian leaders, professional syndicates, and other informal power brokers.
A second domain is budget politics, which focuses on how health financing decisions are embedded within broader fiscal processes. Budget politics analysis examines how health competes with other sectors, how resources are allocated within the health system, and how fiscal crises reshape priorities. In contexts of economic collapse, budget politics often become zero-sum contests, incentivizing selective protection rather than universal coverage.
Leadership politics constitute a third analytical domain. This dimension examines the role of political and bureaucratic leadership in setting reform agendas, managing crises, and navigating opposition. Weak, fragmented, or captured leadership can stall reform even when technical solutions are well understood, while strong leadership can sometimes overcome institutional inertia6.
Finally, external influences play a critical role in shaping health financing in fragile economies. Donors, international financial institutions, and humanitarian agencies often provide funding and technical assistance. While external support can expand fiscal space, it can also distort incentives, reinforce parallel systems, or depoliticize reform debates by framing them as technical compliance exercises rather than political choices (Witter et al., 2019).

Health financing becomes politically instrumentalized when allocation, pooling, and reimbursement decisions are systematically used to manage political risk rather than to protect population health. In such contexts, financing arrangements function as tools for managing political loyalty, deflecting accountability, or preserving elite privilege.
Health financing can serve this function through multiple mechanisms. Fragmented pooling arrangements may allow elites to protect specific constituencies while exposing others to market risk. Selective contracting and reimbursement practices can reward compliant providers and marginalize dissenting ones. Chronic underfunding of public coverage can normalize private out-of-pocket payments--which in Lebanon accounted for over one-third of total health spending even before the crisis--shifting responsibility from the state to households while maintaining the appearance of public provision. In extreme cases, access to publicly financed care becomes contingent on political mediation rather than citizenship or need7.
Weaponization does not require centralized intent. It can emerge from incentive structures that reward fragmentation, discretion, and opacity. When political survival depends on patronage rather than performance, and accountability mechanisms are weak, health financing systems may evolve in ways that systematically undermine solidarity. From a political economy perspective, such outcomes are predictable responses to underlying power configurations.
This framework provides the conceptual foundation for examining Lebanon’s health financing collapse as a politically mediated process rather than a purely technocratic failure.

Chapter Two
Historical and Structural Background of Lebanon’s Health Financing System
Lebanon’s health financing system prior to the 2019 economic collapse reflected long-standing policy choices embedded in a political economy that privileged private provision, fragmented social protection, and discretionary state intervention. While the system delivered acceptable outcomes, it did so at the expense of equity, financial protection, and institutional coherence--rendering it structurally fragile and acutely vulnerable to economic shock.
Pre-crisis health financing structure
Before 2019, Lebanon’s health system was dominated by private providers alongside fragmented public financing arrangements. Private hospitals and clinics delivered the majority of inpatient and outpatient services, while public provision remained limited, under-resourced, and residual8. Recent scoping reviews confirm that this delivery model produced high service availability for insured groups but entrenched inequities, weak public stewardship, and limited system resilience9.
Financing mirrored this fragmentation. Multiple public and quasi-public schemes operated in parallel with minimal coordination and no unified pooling mechanism. The National Social Security Fund (NSSF) covered formally employed private-sector workers; the Cooperative of Civil Servants (COOP) insured public-sector employees; military and security agencies operated separate schemes for their personnel. Individuals without formal coverage--estimated at nearly half the population--were nominally covered by the Ministry of Public Health (MoPH), which acted as payer of last resort by contracting private hospitals for inpatient care10. Prior to the crisis, an estimated 45 - 50% of residents lacked formal insurance coverage, relying on the MoPH’s discretionary hospital contracting for inpatient care.
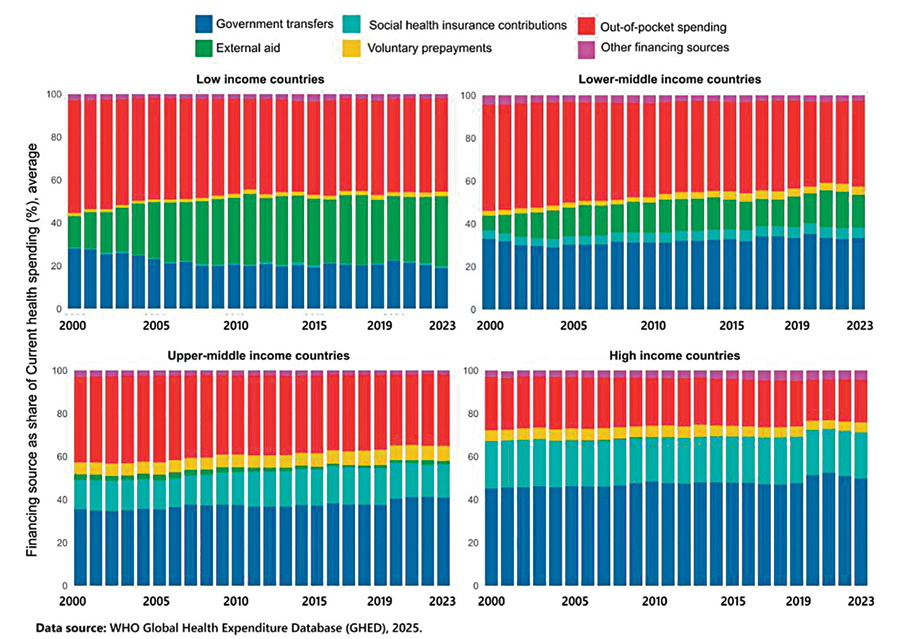
Fig 1: Health Financing Sources in Lebanon (Pre-2019)
This structure illustrates how Lebanon combined relatively high aggregate health spending with minimal effective risk pooling. In practice, this arrangement entrenched segmentation. Each scheme differed in contribution bases, benefit packages, reimbursement rates, and governance arrangements, resulting in limited cross-subsidization between income groups or risk pools. Fragmentation weakened the state’s purchasing power, constraining its ability to regulate prices, enforce quality standards, or strategically contract providers (Kronfol, 2006). From a political economy perspective, fragmentation preserved elite control over specific funds and constituencies while avoiding redistributive pooling that could provoke political resistance.
The MoPH’s role as insurer of last resort was structurally weak. Although it financed a large share of hospital admissions, its budget was politically negotiated and chronically delayed. Reimbursement arrears frequently exceeded 12 - 24 months even before 2019--a duration well beyond standard public payment cycles--fostering informal bargaining between providers and political intermediaries and creating persistent liquidity crises for hospitals (AUB-FHS, 2020). This blurred the boundary between public financing and political mediation, embedding discretion into routine financing practices.
Structural fragility: confessionalism, patronage, and regulation
Health financing arrangements cannot be separated from Lebanon’s confessional political system. Comparative political economy analyses of non-communicable disease prevention in Lebanon similarly demonstrate how policy inertia reflects elite incentives, fragmented authority, and weak accountability rather than technical knowledge gaps11.
Power-sharing institutionalized sectarian representation across state institutions, including ministries, public funds, and regulatory bodies. While intended to preserve balance, this system fostered patronage-based governance in which access to public goods--including healthcare--was mediated through political and sectarian networks12.
In the health sector, these dynamics manifested in limited regulatory autonomy and decision-making processes shaped by broader political considerations. Regulatory bodies faced constraints in independence and enforcement capacity, while licensing, contracting, and reimbursement decisions were often influenced by negotiated arrangements within the political system. Private providers developed close relationships with political actors to navigate contracting processes, payment delays, and regulatory oversight. Over time, health service provision became embedded within informal mediation structures, reinforcing patterns of dependence between service access and political intermediation (Salti & Chaaban, 2010; Kronfol, 2006; Kelsall, 2018).
This governance environment undermined the state’s capacity to act as a strategic purchaser. Instead of using financing mechanisms to shape provider behavior, the state largely accommodated provider interests. Hospital tariffs were adjusted through political negotiation rather than cost analysis, and enforcement of accreditation standards was inconsistent (Kronfol, 2006).
From a political economy perspective, Lebanon’s health financing system displayed features of concentrated decision-making and asymmetric influence. Benefits accrued to groups with political leverage, while costs were shifted onto households through out-of-pocket payments. Institutional fragmentation impeded collective reform efforts, as each fund and constituency defended its privileges. Attempts to unify insurance schemes or expand pooling repeatedly stalled--not due to technical infeasibility, but because they threatened entrenched political equilibria and
patronage-based control (Salti & Chaaban, 2010).
Chronic inequalities and access gaps
The consequences of this model were evident well before the economic crisis. Lebanon consistently recorded one of the highest shares of
out-of-pocket (OOP) health expenditure in the region, accounting for approximately 33 - 40% of current health expenditure13.
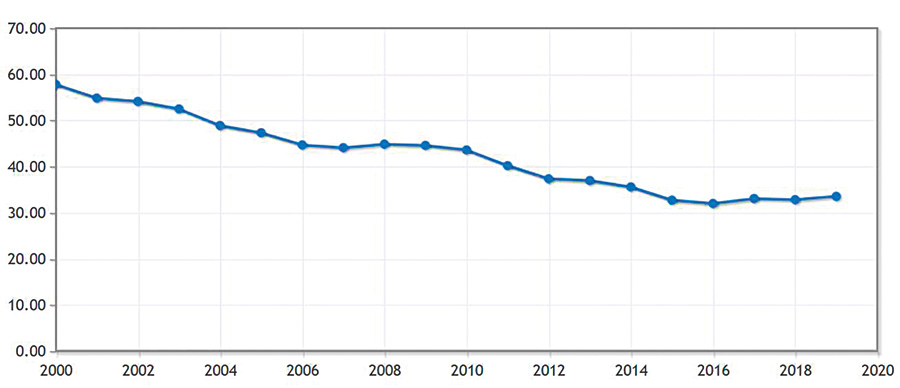
Fig 2: Lebanon out-of-pocket expenditure (% of current health expenditure)
These burdens were unevenly distributed. Individuals covered by NSSF, COOP, or military schemes enjoyed relatively comprehensive benefits, while the uninsured faced limited coverage largely confined to inpatient care. Outpatient services, diagnostics, and pharmaceuticals were predominantly financed out of pocket, disproportionately affecting low-income households and those in informal employment (AUB-FHS, 2020). Geographic disparities further compounded inequity, with rural and peripheral regions experiencing poorer access.
Studies documented delayed care-seeking, reliance on informal payments, and household indebtedness due to health costs (Salti & Chaaban, 2010). Yet these patterns were normalized rather than contested. Private spending was implicitly accepted as compensation for public underinvestment, reducing political pressure for reform and habituating households to individualized risk-bearing. Inequality thus became self-reinforcing: protected groups lacked incentives for pooling reforms, while excluded groups lacked political leverage.
The economic crisis since 2019
The economic collapse beginning in 2019 shattered the fragile equilibrium sustaining Lebanon’s health financing system. Following years of fiscal mismanagement, the country entered a period of banking collapse, sovereign default, and currency freefall. The Lebanese pound lost over 95 percent of its value, inflation surged, and public revenues collapsed. Public health budgets denominated in local currency thus lost over 90% of their real purchasing power. By 2022, more than 80 percent of the population lived in multidimensional poverty14.
Health financing deteriorated rapidly. Public budgets lost real value, rendering MoPH allocations insufficient to cover contracted services. Reimbursement delays intensified, pushing hospitals into financial distress. Insurance contributions collected in local currency became nearly worthless, undermining NSSF and other schemes. Private providers increasingly demanded cash or foreign currency, shifting costs directly onto patients15.
Rather than triggering emergency pooling or protective reforms, the crisis accelerated fragmentation and informalization. Coverage gaps widened as households exited formal employment, and the MoPH’s payer-of-last-resort function became increasingly symbolic. Humanitarian actors filled gaps through parallel mechanisms, further fragmenting financing arrangements16.
Scarcity intensified distributive conflict, reinforcing incentives for selective protection and political mediation. Health financing became increasingly discretionary, with access often contingent on personal networks rather than entitlements. Solidarity collapsed--not merely because resources disappeared, but because the system lacked the institutional and political foundations to sustain collective risk-sharing under stress.

Chapter Three
Mechanisms of Collapse: Politics, Interests, and Financing
The collapse of Lebanon’s health financing system after 2019 did not unfold as a uniform or purely technical failure. Instead, it followed discernible political and institutional pathways that reflected pre-existing power relations and incentive structures. As fiscal space evaporated, health financing became an arena of intensified contestation.
Political capture of health financing
Political capture played a central role in shaping health financing outcomes during the crisis. In Lebanon, budgetary processes are not technocratic exercises but deeply politicized negotiations embedded within a confessional power-sharing system. Health spending competes with other sectors not on the basis of social return but political salience (Salti & Chaaban, 2010; AUB-FHS, 2020). As public revenues collapsed, this politicization intensified. Between 2019 and 2022, the real value of the Ministry of Public Health budget fell by an estimated 70 - 80%, once inflation and currency depreciation are accounted for, based on MoF budget execution and Consumer Price Index adjustments, while no formal emergency pooling mechanism was introduced.
The Ministry of Public Health’s budget illustrates this dynamic. While the MoPH remained nominally responsible for financing care for the uninsured, its allocations were repeatedly eroded in real terms due to inflation and currency depreciation. Budget adjustments failed to keep pace with rising costs, yet no comprehensive emergency pooling or reprioritization mechanism was introduced. Instead, financing decisions became increasingly discretionary, with ad hoc payments, delayed reimbursements, and selective contracting becoming the norm (Bou Sanayeh & El Chamieh, 2023). Hospitals with stronger institutional or relational leverage were better positioned to negotiate payments or secure temporary relief, while less connected facilities faced closure or service reduction.
Regulatory capture further compounded these dynamics. The state’s already limited capacity to regulate prices, enforce contracts, or discipline providers weakened as oversight institutions lost financial and human resources. Several senior decision-makers maintained direct or indirect ties with private healthcare providers, reducing incentives to impose cost controls or restructure purchasing arrangements that could disrupt established relationships (Kronfol, 2006). As a result, the burden of adjustment shifted downward to households through higher out-of-pocket payments, informal fees, and exclusion from care.
From a political economy perspective, this pattern reflects capture dynamics that emerge under conditions of acute scarcity. Rather than reallocating limited resources to enhance protection for the most vulnerable, financing arrangements preserved discretionary control over resource flows, enabling decision-makers to manage political exposure while shifting adjustment costs onto households. Health financing did not simply “shrink”; it reallocated and rationed in ways consistent with prevailing power structures.
Fragmentation and exclusion
Fragmentation--long a defining feature of Lebanon’s health financing system--became a primary mechanism of exclusion during the crisis. Formal insurance funds such as the NSSF saw their contribution base collapse as unemployment surged and wages lost real value. Benefits remained nominally intact but increasingly meaningless in practice, as reimbursement rates failed to match provider costs17.
At the same time, the MoPH’s role as payer of last resort deteriorated sharply. Budgetary constraints and reimbursement delays forced hospitals to restrict admissions of MoPH-covered patients or demand upfront payments, effectively nullifying coverage for many uninsured individuals (MSF, 2022). In effect, coverage existed on paper but not in reality--a phenomenon widely documented in fragile health systems (Witter et al., 2019).
The private sector’s role in this process was pivotal. Private hospitals and suppliers, operating in a dollarized cost environment, adjusted rapidly to protect their financial viability. Pricing in foreign currency, requiring cash payments, and prioritizing privately insured or self-paying patients became survival strategies. While these actions were economically rational at the provider level, they reinforced exclusionary dynamics and widened access gaps.

Fragmentation thus evolved from a structural weakness into an active mechanism of exclusion. Instead of consolidating pools or harmonizing benefits to manage crisis risk collectively, the system allowed fragmentation to determine who absorbed the shock. Those with access to foreign currency, political mediation, or elite insurance schemes retained access to care; others were effectively priced out. Solidarity fractured along pre-existing social and economic lines.
Patronage and clientelism
Patronage and clientelism provided the connective tissue linking political capture and fragmentation. In Lebanon, access to public services has long been mediated through personal and sectarian networks, and healthcare is no exception (Salti & Chaaban, 2010). During the crisis, these informal mechanisms intensified as formal entitlements weakened.
Access to hospital care, fee adjustments, or essential medications was often facilitated through intermediated channels rather than standardized entitlement processes. While these mechanisms occasionally mitigated immediate hardship for individuals, they weakened rights-based access and reinforced reliance on discretionary intervention. As a result, allocation patterns became less aligned with population health needs and more dependent on individualized pathways of access.
Crucially, patronage thrived precisely because formal financing mechanisms failed. As MoPH coverage became unreliable and insurance benefits eroded, households increasingly sought political mediation to access care (Kelsall, 2018).
External actors and conditionality
Donors, humanitarian agencies, and international financial institutions provided critical support during the crisis, particularly in areas such as primary care, pharmaceuticals, and emergency response. However, their interventions also interacted with domestic political dynamics in ways that sometimes reinforced fragmentation.
Humanitarian actors, including NGOs and UN agencies, expanded parallel service delivery and financing mechanisms to compensate for state failure. While these efforts were essential for maintaining access to care, they often bypassed national pooling arrangements and accountability structures (MSF, 2022). Over time, this parallelization normalized state withdrawal and reduced pressure for systemic reform--a pattern well documented in fragile and conflict-affected settings (Witter et al., 2019).
International financial institutions, particularly the IMF, emphasized macroeconomic stabilization and fiscal consolidation as prerequisites for assistance. While defensible from a macroeconomic perspective, these conditions constrained fiscal space for social spending in the short term. In the absence of strong domestic political commitment to protect health financing, macroeconomic adjustment pressures further constrained public coverage (World Bank, 2022). Importantly, conditionality did not create fragmentation, but it operated within and reinforced existing political incentives to shift costs onto households.
Political economy analysis cautions against viewing external influence as either benevolent or malign in isolation. What matters is how external resources and conditions interact with domestic power structures. In Lebanon’s case, external actors mitigated humanitarian collapse but did not alter the political equilibrium governing health financing. As a result, emergency assistance substituted for solidarity rather than restoring it.
Crisis amplification: overlapping shocks
Finally, overlapping crises amplified all the mechanisms described above. The Beirut port explosion in August 2020 destroyed major health infrastructure, increased demand for emergency care, and imposed additional fiscal burdens on an already collapsing system. The COVID-19 pandemic further strained financing, forcing reallocations without expanding fiscal space (Bou Sanayeh & El Chamieh, 2023).
Lebanon’s long-standing refugee presence added another layer of complexity. While international funding supported refugee health services, these arrangements often operated in parallel to national systems, reinforcing segmentation. The cumulative effect of economic collapse, pandemic, explosion, and displacement was not merely additive--it was multiplicative. Each crisis reinforced reliance on discretionary financing, patronage, and external assistance, accelerating the erosion of collective mechanisms.
These crises revealed political priorities with unusual clarity. Where emergency resources were mobilized, they flowed through channels that preserved discretionary authority and existing power balances. Where universal protection would have required institutional reform, inaction prevailed. The collapse of health financing thus emerged not as a failure of foresight, but as the predictable outcome of a political system
ill-equipped--and insufficiently motivated--to sustain solidarity under pressure.

Chapter Four
Consequences: The Erosion of Solidarity
The political and institutional mechanisms produced a set of consequences that fundamentally altered the social meaning and functioning of Lebanon’s health system. At the center of these outcomes lies the collapse of
solidarity--the principle that health risks should be collectively shared and publicly mediated rather than individualized and marketized. This section examines the consequences of that displacement across four dimensions: risk pooling, equity and access, system performance, and public trust.
Collapse of risk pooling
Risk pooling is the institutional expression of solidarity in health financing. When pooling functions effectively, financial risk is redistributed across populations, protecting individuals from catastrophic expenditure. In Lebanon, the crisis rendered risk pooling mechanisms largely ineffective. Insurance schemes such as the NSSF continued to exist formally, but their capacity to pool risk collapsed as contributions lost real value and benefits became disconnected from provider pricing (WHO, 2022; Bou Sanayeh & El Chamieh, 2023).
As public financing eroded, out-of-pocket payments surged, becoming the dominant mode of health financing for many households. After 2019, OOP payments became the default means of access for services ranging from diagnostics to hospitalization (AUB-FHS, 2020). Providers increasingly required upfront payment, often in foreign currency, effectively excluding individuals without liquid resources. Households assumed direct financial responsibility for risks previously mediated--however imperfectly--by public or quasi-public schemes.
This collapse of pooling had predictable consequences. Households delayed or forewent care, rationed medications, and relied on informal coping strategies, including borrowing and asset sales (MSF, 2022; WHO, 2022). Catastrophic health expenditure, already prevalent, became normalized. Household surveys conducted before the crisis already estimated catastrophic health expenditure incidence at 8 - 10% of households;
post-2019, available evidence suggests this figure rose sharply, particularly among uninsured and informal workers, though comprehensive national data are lacking due to the breakdown of routine household surveys. Solidarity was no longer embedded in institutions; it was replaced by individualized survival strategies.
Social inequities and health access outcomes
The erosion of solidarity translated directly into widening social inequities in health access. While the crisis affected all segments of Lebanese society, its impact was profoundly unequal. Individuals with access to foreign currency, private insurance, or political connections retained relative continuity of care. By contrast, low-income households, informal workers, and those dependent on MoPH coverage experienced severe access barriers (AUB-FHS, 2020).

Disparities between Lebanese citizens and refugee populations further illustrate this dynamic. Refugees, particularly Syrians, relied heavily on humanitarian financing mechanisms that operated in parallel to national systems. While these arrangements provided essential services, they also reinforced segmentation by nationality and legal status. Access to care became governed by eligibility criteria tied to donor programs rather than universal entitlement, entrenching differential treatment within the same geographic space (MSF, 2022). Solidarity fractured not only along class lines but also along citizenship and displacement status.
These inequities were not incidental. They reflected the underlying financing architecture, which lacked mechanisms to redistribute resources spatially or socially under stress. In the absence of strong pooling and purchasing functions, inequity became the system’s default outcome. From a political economy perspective, this outcome was tolerated and insufficiently countered because those most affected lacked political leverage to demand corrective action.
Systemic performance declines
The erosion of solidarity also had severe implications for system performance. Hospitals and clinics faced escalating operational costs due to dollarized inputs, supply chain disruptions, and workforce attrition. By 2022, multiple hospitals had closed wards or suspended services, while others operated at 50% capacity or less. Public reimbursement delays and underpayment pushed many facilities into financial insolvency, leading to service reductions or closures (Bou Sanayeh & El Chamieh, 2023).
Hospital closures were not evenly distributed. Facilities serving poorer populations or heavily reliant on MoPH payments were particularly vulnerable, reinforcing access inequities. Even surviving hospitals reduced capacity, closed specialized units, or limited admissions. Essential services such as oncology, dialysis, and chronic disease management were disrupted, with long-term consequences for population health.

Health workforce emigration represented one of the most damaging systemic consequences. Between 2019 and 2023, professional orders estimate that 30 - 40% of nurses and a significant share of early-career physicians left the country. This “brain drain” further weakened service delivery and institutional memory, creating a vicious cycle in which declining quality accelerated demand for private or external alternatives (WHO, 2022).
Shortages of medicines and medical supplies compounded these challenges. Currency controls and import barriers disrupted pharmaceutical supply chains, forcing patients to pay exorbitant prices or forgo treatment. While ad hoc subsidy schemes were introduced, they were inconsistently implemented and often captured by intermediaries18.
Collectively, these performance declines illustrate how the erosion of solidarity undermines not only equity but efficiency. Without collective financing and strategic purchasing, the system lost its capacity to plan, prioritize, and sustain service delivery. Crisis management replaced governance, and survival replaced stewardship.
Public trust and legitimacy deficit
Perhaps the most consequential outcome of the collapse of solidarity is the erosion of public trust. In Lebanon, the health financing collapse reinforced public perceptions of state abandonment, corruption, and inequality (AUB-FHS, 2020).
As formal entitlements became unreliable, households increasingly relied on informal networks, charitable organizations, or political patrons to access care. While these mechanisms provided temporary relief, they further delegitimized public institutions. The state was no longer perceived as a guarantor of basic welfare but as an arena of contestation and favoritism.
Trust erosion has long-term implications. Low trust reduces compliance with public health measures, undermines willingness to contribute to insurance schemes, and weakens support for reform. In fragile states, once trust collapses, rebuilding solidarity becomes exponentially more difficult, as citizens no longer believe that collective arrangements will protect them (Witter et al., 2019).
Taken together, these consequences demonstrate that the erosion of solidarity was not an abstract ethical concern but a concrete determinant of health outcomes, system performance, and political legitimacy. The next section situates Lebanon’s experience within a broader comparative perspective, highlighting how similar dynamics unfold in other fragile economies--and what, if anything, distinguishes the Lebanese case.

Chapter Five
Comparative Perspectives from Fragile Economies
Lebanon’s health financing collapse is often portrayed as exceptional, driven by an unprecedented financial meltdown layered onto long-standing political dysfunction. While the severity of Lebanon’s crisis is indeed extreme, the underlying political economy mechanisms shaping health financing outcomes are not unique. Comparative research on fragile and conflict-affected settings shows that health financing outcomes are shaped less by technocratic design than by power relations, elite incentives, and crisis-driven political calculations (Witter et al., 2017; Kutzin et al., 2018). Situating Lebanon within this comparative literature allows for a clearer distinction between generalizable patterns of fragility and the specific configurations that render the Lebanese case particularly acute19.
Fragile contexts beyond Lebanon
Fragility does not simply reduce the technical capacity of health financing systems; it fundamentally reshapes the incentive environment in which they operate. Across fragile and conflict-affected states, health financing evolves under conditions of institutional weakness, fiscal volatility, and contested authority. In such contexts, formal financing arrangements – such as social insurance schemes, tax-based funding, or pooled donor mechanisms – often coexist with informal practices, parallel delivery systems, and discretionary allocation of resources (Witter et al., 2019).
Research from settings such as Afghanistan, South Sudan, the Democratic Republic of Congo, and Yemen highlights how political settlements fundamentally shape health financing trajectories. Where elites view health financing as a tool for legitimacy-building, limited pooling and subsidization may be expanded selectively. Where health is perceived as politically marginal or risky, financing is neglected or outsourced to donors and non-state actors (Kelsall, 2018; Witter et al., 2017). In such contexts, health financing functions more as a political instrument than as a social contract.
Donor dominance is a defining feature of many fragile contexts. External financing often fills fiscal gaps but introduces its own political economy distortions. Donor-funded vertical programs, humanitarian exemptions, and parallel purchasing arrangements can temporarily expand access while undermining national pooling and state stewardship in the long term20. In such cases, solidarity is redefined not as a national principle but as a humanitarian or project-based commitment--time-bound, conditional, and externally governed21.
Comparative mechanisms: politics, fragmentation, and crisis incentives
When examined comparatively, three recurring mechanisms emerge across fragile health financing systems: political capture, fragmentation, and crisis-induced incentive distortion. These mechanisms are not identical to Lebanon’s experience, but they follow a similar structural logic.
Political capture manifests when decision-making authority over health resources becomes concentrated within narrow institutional or administrative channels. In several settings, health budgets have consistently favored high-cost tertiary facilities and hospital-based care, while primary care services and risk-pooling mechanisms remain underfunded (Kutzin et al., 2018). As a result, financing decisions tend to reflect considerations of operational control and immediate service continuity rather than population health needs or long-term financial protection.
Fragmentation is both a cause and consequence of political capture. Multiple insurance schemes, donor programs, and informal payment arrangements proliferate in the absence of strong central authority. It systematically undermines pooling and equity. Comparative studies show that fragmented financing systems in fragile states tend to entrench segmentation by income, geography, and political affiliation (Witter et al., 2019).

Crisis incentives further distort financing behavior. In fragile settings, recurrent shocks--conflict, epidemics, displacement, macroeconomic collapse--reward short-term fixes over institutional reform. Emergency funding bypasses national systems, discretionary exemptions replace entitlement-based coverage, and political leaders gain visibility through crisis response rather than system-building. Over time, crisis becomes the organizing logic of health financing (Bertone & Witter, 2021).
These mechanisms interact dynamically. Political capture fuels fragmentation; fragmentation amplifies vulnerability to crisis; crisis, in turn, strengthens elite incentives to avoid consolidation. The result is a low-equilibrium health financing system that is remarkably resilient to reform but highly vulnerable to collapse.
What differentiates Lebanon?
While Lebanon shares these mechanisms with other fragile economies, three factors distinguish its experience and help explain the depth and speed of its health financing collapse.
First, the depth and institutionalization of informal allocation mechanisms in Lebanon exceed those observed in many fragile contexts. Unlike post-conflict settings where authority is fragmented territorially or administratively, Lebanon’s governance system is formally stable but characterized by highly segmented decision-making structures. Health financing institutions were embedded from their inception within negotiated allocation arrangements across multiple authorities. As a result, financing fragmentation was not a temporary response to fragility, but a durable structural feature of system design (Kronfol, 2006).
Second, the severity and simultaneity of economic collapse sharply differentiate Lebanon. The scale and simultaneity of monetary, banking, and income collapse are unusual even among fragile economies. This collapse directly eroded contribution-based financing and rendered public reimbursement mechanisms non-functional almost overnight. In other fragile contexts, donor inflows or natural resource rents often partially buffer such shocks; in Lebanon, they did not.
Third, Lebanon’s health system is characterized by a highly privatized service delivery model embedded within weak public financing. In many fragile states, public provision dominates despite quality constraints. In Lebanon, private providers form the backbone of service delivery, but rely heavily--if unevenly--on public and quasi-public financing. When financing collapsed, the private sector did not substitute for the state; it priced itself out of reach. This hybrid model amplified exclusion rather than mitigating it. As a result, financing collapse translated rapidly into access collapse.
A further distinguishing factor is Lebanon’s long-standing integration into global medical markets--through pharmaceutical imports (though there was a shift toward local manufacturing during the crisis), medical tourism, and internationally mobile health professionals--magnified the system’s exposure to currency collapse. Dollarization of inputs combined with local-currency reimbursement created structural insolvency across the sector, accelerating workforce exit and service contraction (WHO, 2022).
Taken together, these factors suggest that Lebanon represents an extreme case: a fragile political settlement operating within a middle-income, highly medicalized health system that collapsed not through armed conflict but through political economy failure. This configuration exposes the limits of prevailing UHC and resilience frameworks when solidarity is not merely weak but politically expendable. It also challenges assumptions that private sector depth compensates for weak public financing--a claim often implicit in middle-income health reform narratives.
The comparative perspective thus reinforces the central claim that health financing collapse in fragile economies is not primarily a technical failure but a political outcome. Lebanon’s experience demonstrates how patronage, fragmented financing, and crisis-driven incentives can transform health financing from a mechanism of social protection into a vector of exclusion. The final section turns to the implications of this analysis for reform, asking whether--and under what conditions--solidarity can be reconstructed in such contexts.

Chapter Six
Pathways to Reform and Restoring Solidarity
Because Lebanon’s health financing collapse is fundamentally political, pathways to reform must be evaluated through political economy rather than technical feasibility alone. Restoring solidarity in such a context is not a matter of redesigning benefit packages or recalibrating provider payment mechanisms. It requires altering incentives, constraining discretionary power, and rebuilding collective arrangements. Potential reform pathways do exist, but their political limits must be acknowledged explicitly.
Political economy–informed reforms
The first implication of the analysis is that sequencing matters more than design. Comprehensive health financing reform--such as unified insurance, expanded tax-based pooling, or strategic purchasing--is politically infeasible in Lebanon’s current incentive structures. Attempting such reforms prematurely risks symbolic adoption without implementation, elite capture under the guise of reform.
Instead, politically informed reform must begin with coalition-building around partial solidarity gains focused on system stabilization rather than redistribution. Such coalitions emerge by aligning actors around shared operational risks rather than normative commitments. Hospital associations, professional syndicates, pharmaceutical importers, and middle-income contributors are all exposed to financing volatility through delayed reimbursements, currency mismatch, supply disruptions, and workforce instability.
Coalition-building occurs through narrow, issue-specific convergence on objectives such as predictable reimbursement timelines, minimum budget guarantees for public purchasing, and standardized payment rules. These demands reduce uncertainty without requiring unified risk pooling. Advanced through professional bodies, technical forums, or regulatory processes, they avoid triggering resistance associated with broader reform agendas.
Transparency in budgeting and reimbursement constitutes a second entry point. Lebanon’s health financing collapse has been exacerbated by opaque allocation processes and discretionary payment practices. Introducing publicly accessible budget execution data, standardized reimbursement schedules, and rule-based payment timelines would not eliminate patronage but would raise its transaction costs. Political economy research suggests that even modest transparency reforms can shift incentives by narrowing elite discretion and enabling contestation (Kutzin et al., 2018). Transparency functions here not as a governance ideal, but as a political constraint on discretion.
Progressive pooling must be approached defensively rather than expansively. In the short term, this does not mean national insurance unification. It means protecting and partially recapitalizing existing pooling arrangements--particularly MoPH coverage--through earmarked revenues (noting constitutional constraints) or externally backed stabilization funds.
Crucially, financial protection must be accompanied by governance convergence. While pools may remain institutionally separate, they should operate under unified governance standards for eligibility, benefit definition, reimbursement rules, and payment timelines. Such standardization limits discretionary variation across schemes, reduces opportunities for selective treatment, and creates de facto coordination without formal consideration.
The objective is not immediate redistribution but containment, preventing further individualization of risk and restoring predictability to financing relationships. Without stabilizing both funding flows and governance rules, solidarity cannot be rebuilt later.
Reform efforts must avoid technocratic overreach. Policies that assume administrative capacity or political neutrality--such as complex purchasing reforms or performance-based financing--are unlikely to survive Lebanon’s institutional environment. Political economy-informed reform prioritizes robustness over elegance. In such contexts, technically “best” reforms are often politically worst.

Global frameworks and accountability
Global health frameworks, particularly those promoted by the World Health Organization, offer useful analytical tools but limited leverage unless adapted to domestic political realities. WHO’s political economy analysis framework emphasizes stakeholder mapping, power analysis, and reform feasibility under constraint (WHO, 2022). This approach shifts the focus from “what should be done” to “what can be sustained politically.”
In Lebanon, such tools can be used to reframe reform narratives. Rather than presenting solidarity as a moral imperative, reform advocates can position it as a system-stabilizing function that reduces fiscal unpredictability, provider insolvency, and social unrest. This reframing aligns solidarity with elite risk management rather than redistribution alone.
External actors also play a critical accountability role, though their influence is double-edged. In Lebanon, however, this role has been inconsistently exercised. Donors and international financial institutions have often reinforced fragmentation through project-based financing and conditional humanitarian exemptions. By 2021, externally funded health expenditures accounted for an estimated 25 - 30% of total health spending, much of it channeled outside national pooling mechanisms. To support solidarity, external assistance must be tied not to austerity targets alone but to institutional safeguards for pooling and entitlement. This includes protecting health budgets from arbitrary cuts, ensuring currency adjustment mechanisms for providers, and resisting the proliferation of parallel financing channels.
However, global frameworks cannot substitute for domestic accountability. Without local actors capable of contesting capture and demanding
rule-based financing, external leverage will remain temporary. Political economy evidence from fragile states suggests that donor-driven reform momentum dissipates once conditionality weakens or crises recede (Witter et al., 2019).
Risks and political obstacles
Any pathway to restoring solidarity must confront three structural obstacles that cannot be wished away.
First, resistance to health financing reform is best understood as
incentive-driven rather than anomalous. Fragmented financing arrangements create discretion and operational predictability for key institutional actors, which reforms inevitably disrupt. Expecting solidarity-based change without adjusting these incentives misreads how governance systems function. Effective reform must therefore reduce discretionary space and formalize rules, rather than rely on normative appeals that lack institutional enforcement.
Second, short political and crisis cycles undermine long-term reform. In an environment of recurrent shocks--economic instability, security threats, humanitarian crises--political attention gravitates toward immediate containment. Structural reform, which produces diffuse and delayed benefits, is systematically deprioritized.
Third, institutional weakness limits absorptive capacity. Even politically feasible reforms risk failure if administrative systems cannot implement them. Weak information systems, limited enforcement capacity, and politicized bureaucracy jointly constrain implementation capacity. Overloading institutions with complex reform agendas increases the likelihood of symbolic compliance and practical collapse.
These obstacles imply that restoring solidarity is not a linear process. Partial gains may be reversed; reform windows may close abruptly. The realistic objective is not transformation but reversal of downward spirals--reestablishing minimum pooling, predictable financing flows, and credible entitlement, even at low coverage levels.
Ultimately, solidarity in fragile political economies cannot be engineered solely through policy instruments. It emerges when collective arrangements become less risky than individualized strategies--for households, providers, and political actors alike. Whether Lebanon can reconstruct that contract remains uncertain--but without confronting the political logic that dismantled solidarity, reconstruction is structurally impossible. What is clear, however, is that without confronting the political economy of health financing head-on, reform efforts will continue to oscillate between technical sophistication and practical irrelevance.
Conclusion
Lebanon’s health financing collapse reveals a deeper lesson about how systems fail under pressure. The breakdown was not triggered solely by economic shock, nor can it be explained by technical weaknesses alone. Rather, it reflects a structural condition in which financing arrangements were never designed to function as instruments of collective protection. When stress arrived, the system did not bend--it reverted to its underlying logic. What collapsed was not only funding flows or service delivery, but the expectation that health risk would be managed collectively and predictably.
This experience underscores a critical distinction between systems that operate and systems that endure. Health financing arrangements may appear functional during periods of relative stability, even when they are fragmented and discretionary. Services are delivered, expenditures are high, and outcomes may seem acceptable for significant segments of the population. Yet resilience is not tested in equilibrium. It is tested when currency collapses, fiscal space disappears, or crisis multiplies demand. Under such conditions, systems built without embedded solidarity do not merely underperform--they reorganize access around exclusion, discretion, and individual coping.
The Lebanese case thus challenges prevailing assumptions in health financing reform. Expanding coverage on paper, increasing spending ratios, or introducing isolated purchasing reforms do not necessarily strengthen collective protection. Where financing institutions lack credible rules, unified governance, and protected pooling mechanisms, reform remains reversible. Technical sophistication can coexist with political fragility, and efficiency gains can evaporate under stress. In this sense, collapse is not an anomaly but a diagnostic moment that exposes what was structurally absent all along.
This perspective invites a shift in how health system fragility is understood. Fragility is not only a matter of conflict, low capacity, or institutional absence. It can also arise from institutional presence without enforceable rules, from financing mechanisms that prioritize flexibility over credibility, and from governance arrangements that reward discretion rather than obligation. Such systems are particularly vulnerable to cascading failure because crisis amplifies the very incentives that undermine solidarity.
For policymakers and external partners, the lesson is not that solidarity must be idealized, but that it must be institutionalized. Emergency financing, humanitarian exemptions, and short-term stabilization measures may preserve access temporarily, but they cannot substitute for durable pooling and entitlement credibility. Without protecting these foundations, crisis responses risk normalizing fragmentation and postponing accountability.
Looking forward, a critical question emerges--one that extends beyond Lebanon and invites further inquiry: what makes health financing arrangements politically durable under stress? Answering this requires moving beyond static indicators of coverage or spending toward a deeper examination of how pooling rules are protected, how entitlements are enforced during crisis, and how governance systems constrain discretionary erosion. The future of health financing research lies not in designing ideal systems, but in understanding which institutional configurations survive when conditions deteriorate.
In that sense, the collapse of solidarity is not only a warning--it is a research frontier.
References
1. Sparkes, Susan P., Jesse B. Bump, Ece A. Özçelik, Joseph Kutzin & Michael R. Reich (2019). Political economy analysis for health financing reform. Health Systems & Reform, 5 (3), 183–194. https://doi.org/10.1080/23288604.2019.1633874
2. World Health Organization (WHO) (2024). Political Economy Analysis for Health Financing: How-to Guide. Geneva: WHO. ISBN 978-92-4-009209-9.
3. Reich, Michael R. & Campos, Paola Abril (2020). Why political analysis is essential for health reform. Health Systems & Reform, 6 (2), e1823886.
https://doi.org/10.1080/23288604.2020.1823886
4. Kutzin, Joseph et al. (2018). Health financing, universal coverage, and health system performance: concepts and implications for policy. Bulletin of the World Health Organization, 96 (9), 602–612.
5. Witter, Sophie, Maria Paola Bertone, Elina Dale & Matthew Jowett (2019). Health financing in fragile and conflict-affected settings: What do we know? Social Science & Medicine, 232, 209–219. https://doi.org/10.1016/j.socscimed.2019.04.019
6. Witter, Sophie et al. (2017). Health systems resilience in fragile and conflict-affected settings. Health Policy and Planning, 32 (Suppl 3), iii1–iii12.
7. Bertone, Maria Paola & Sophie Witter (2021). The political economy of health financing reform in fragile and conflict-affected settings. Health Policy and Planning, 36 (Suppl 2), ii3–ii14.
8. Kelsall, Tim (2018). Thinking and working with political settlements. London: Overseas Development Institute (ODI).
9. BMJ Global Health (2018). Rocha Menocal, Alina et al., Fragile, handle with care: refining a key concept for global health. BMJ Global Health, 3 (Suppl 3), e000984.
10. Kronfol, Nabil (2006). Rebuilding of the Lebanese health care system: health sector reforms. Eastern Mediterranean Health Journal, 12 (3–4), 459–473.
11. Bou Sanayeh, Elie & Carolla El Chamieh (2023). The fragile healthcare system in Lebanon: sounding the alarm about its possible collapse. Health Economics Review, 13, Article 21. https://doi.org/10.1186/s13561-023-00416-x
12. World Health Organization (WHO) (2022). Lebanon Health System Review. Health Systems in Transition, Vol. 24, No. 2.
Margin
1. World Health Organization. Health Systems Financing: The Path to Universal Coverage. World Health Report 2010. Geneva: WHO; 2010.
2. Sparkes, S. P., Bump, J. B., Özçelik, E. A., Kutzin, J., & Reich, M. R. “Political Economy Analysis for Health Financing Reform.” Health Systems & Reform 5, no. 3 (2019): 183–194.
3. North, D. C. Institutions, Institutional Change and Economic Performance. Cambridge: Cambridge University Press, 1990; Reich, M. R., & Campos, P. A. “Why Health Reforms Fail: Political Economy Perspectives.” Health Systems & Reform 6, no. 2 (2020).
4. Bump, J. B. “The Political Economy of Health Systems Reform.” Health Policy and Planning 33, no. 4 (2018): 474 - 487.
5. World Health Organization. Political Economy Analysis for Health Financing Reform, 2024.
6. Reich, M. R., & Campos, P. A. “Why Is Health Reform So Difficult? A Political Economy Perspective.” Health Systems & Reform 6, no. 1 (2020): e1754106.
7. Kelsall, T. Thinking and Working with Political Settlements. ODI, 2018; Witter, S. et al. “Health Financing in Fragile and Conflict-Affected Settings.” Health Policy and Planning 34, Suppl. 2 (2019): ii1–ii7.
8. Kronfol, N. “Rebuilding of the Lebanese Health Care System.” Eastern Mediterranean Health Journal 12, no. 3 - 4 (2006):459 - 473.
9. Healthcare delivery in Lebanon: a critical scoping review of strengths, weaknesses, opportunities, and threats. BMC Health Services Research, 2024.
10. American University of Beirut – Faculty of Health Sciences (AUB-FHS). National Health Statistics Report, 2020.
11. Political Economy of Non-Communicable Disease (NCD) Prevention and Control in Lebanon: Identifying Challenges and Opportunities for Policy Change and Care Provision Reforms. BMC Public Health, 2023.
12. Salti, N., & Chaaban, J. “The Role of Sectarianism in the Allocation of Public Expenditure in Lebanon.” World Development 38, no. 10 (2010): 1436 - 1447.
13. World Health Organization. Global Health Expenditure Database, 2018.
14. World Bank. Lebanon Poverty Assessment, 2022.
15. Bou Sanayeh, J., & El Chamieh, C. “Lebanon’s Health Sector at Risk.” Lebanese Medical Journal 71, no. 2 (2023).
16. Médecins Sans Frontières (MSF). Lebanon: Healthcare Under Pressure, 2022.
17. World Health Organization. Health Financing Diagnostic: Lebanon, 2022.
18. Lebanese Center for Policy Studies (LCPS). The Political Economy of Subsidies in Lebanon, 2023.
19. Witter, S. et al. Health financing in fragile and conflict-affected settings: What do we know? Social Science & Medicine.
20. Bertone, M. P. et al. “Health Financing in Fragile Settings: What Do We Know?” Health Systems & Reform 5, no. 2 (2019).
21. Understanding the political economy of reforming global health initiatives: Insights from global and country levels. Publicly available PMC, indexed article.
مَن قتل التضامن؟ الاقتصاد السياسي لانهيار تمويل الرعاية الصحية في لبنان والدول الهشة
العقيد الصيدلي حبيب عبده
شهد لبنان منذ العام 2019 انهيارًا حادًا في نظام الرعاية الصحية، لم يقتصر على تراجع التمويل أو تدهور الخدمات، بل امتد ليطال الأساس الذي يقوم عليه أي نظام صحي مستدام: التضامن. فعلى الرغم من أن الإنفاق الصحي كان يتجاوز 8% من الناتج المحلي الإجمالي قبل الأزمة، بقيت الحماية المالية ضعيفة، حيث شكّلت المدفوعات المباشرة من جيوب المواطنين ما بين 34% و38% من إجمالي الإنفاق، وهي نسبة ترتبط عالميًا بارتفاع مخاطر الإنفاق الصحي الكارثي.
اتسم النظام الصحي بتجزئة واضحة في آليات التمويل، إذ تعددت الجهات الضامنة بين الصندوق الوطني للضمان الاجتماعي، وتعاونية موظفي الدولة، وأنظمة خاصة بالقوى العسكرية والأمنية، إلى جانب وزارة الصحة التي غطّت نحو نصف السكان ممن لا يملكون تأمينًا رسميًا. هذا التعدد لم يكن مصحوبًا بتنسيق فعّال أو تجميع موحّد للمخاطر، ما أدى إلى تفاوت كبير في التغطية والخدمات. كما هيمن القطاع الخاص على تقديم الخدمات، في ظل دور محدود للقطاع العام وضعف في القدرة التنظيمية والرقابية.
مع تفاقم الأزمة الاقتصادية، فقدت الليرة اللبنانية أكثر من 95% من قيمتها، وتراجعت القدرة الشرائية للموازنات الصحية العامة بأكثر من 90%. في الوقت نفسه، ارتفعت معدلات الفقر لتشمل أكثر من 80% من السكان بحلول العام 2022. انعكس ذلك مباشرة على تمويل الرعاية الصحية، حيث أصبحت التغطية النظرية غير كافية عمليًا، وازدادت الفجوة بين كلفة الخدمات وقدرة الأفراد على تحمّلها. لجأت المؤسسات الصحية إلى فرض الدفع النقدي، غالبًا بالعملة الأجنبية، ما أدى إلى إقصاء شريحة واسعة من السكان.
ترافقت هذه التطورات مع تراجع في الأداء النظامي، تمثّل في إغلاق أقسام في المستشفيات، وانخفاض القدرة التشغيلية، وهجرة الكوادر الصحية، حيث غادر ما بين 30% و40% من الممرضين وعدد كبير من الأطباء الشباب البلاد. كما تفاقمت أزمة توافر الأدوية نتيجة اضطراب سلاسل الإمداد وارتفاع الأسعار، ما أجبر المرضى على تقليص العلاج أو التخلّي عنه.
في هذا السياق، تراجعت آليات تقاسم المخاطر بشكل كبير، وتحوّل تمويل الرعاية الصحية إلى عبء فردي. لم يعد الوصول إلى الخدمات الصحية يعتمد على الحقوق أو الحاجة، بل على القدرة المالية أو الوسائل غير الرسمية لتأمين الخدمة. كما برزت أنماط موازية من التمويل والخدمات مدعومة من جهات خارجية، أسهمت في سد فجوات آنية، لكنها عززت في الوقت نفسه من تجزئة النظام.
تُظهر هذه المعطيات أن وجود خدمات صحية متقدمة نسبيًا لا يضمن بالضرورة تحقيق العدالة أو الاستدامة، خاصة في غياب قواعد واضحة للحوكمة وآليات فعالة لتجميع الموارد. فحين تغيب هذه الأسس، تصبح الأنظمة عرضة للتآكل السريع عند التعرض للصدمات.
في ضوء ذلك، يبرز تساؤل محوري للمستقبل: ما الذي يجعل أنظمة تمويل الرعاية الصحية قادرة على الصمود في وجه الأزمات؟ يرتبط الجواب بمدى قدرة هذه الأنظمة على الحفاظ على آليات تقاسم المخاطر، وضمان استمرارية التغطية، وترسيخ قواعد حوكمة تحدّ من التفاوت وتدعم الاستقرار، حتى في أكثر الظروف صعوبة.
